

Though it was somewhat in jest, hearing sleep physician colleagues refer to oral appliance therapy as “the black hole of sleep apnea treatment” stung, concedes Charles Tozzer, DDS, co-owner of Sleep Apnea Centers of California. “I was pleased with our results, but it just took too long. I thought maybe we could make this work a little better.”
Using new technology-enabled protocols, Tozzer and others have streamlined oral appliance steps from start to finish, emerging from the black hole with a data-guided path clinicians can follow in real time. Use their strategies to help your patients reach their optimal oral appliance position in days or weeks rather than months, all while minimizing the risk of side effects like temporomandibular joint (TMJ) discomfort.
Better Bites
Construction bite midline errors are common, according to Michael Murray, DDS, DABDSM, founder of The Sleep Apnea Center of Connecticut. Worse, when a lab identifies a discrepancy, the dentist must decide whether it’s worth the time to bring the patient back in to redo the bite scans, potentially adding weeks to the delivery date.
To catch discrepancies earlier, Murray developed a protocol using Medit intraoral scanning software to identify midline shifts while the patient remains in the chair. The software’s multi-occlusion function lets the dentist verify the midline in the maximum intercuspation position. Similar to how a comic flipbook simulates motion, switching between two occlusal digital scan images lets the dentist visualize the movement of the lower jaw and the midline position. “I could see if the mandible is actually shifting to the left or right. I can correct that before I even submit my scan to the lab,” Murray says.
His practical protocol, presented at the AADSM and SLEEP 2025 meetings, found that seven out of 10 patients had midline construction bite discrepancies only caught because of this digital verification.1 “It only adds maybe 30 seconds to the visit, but the time you would save in having to bring the patient back—also the increased efficacy of less side effects and less discomfort by doing it this way—pays off.”
Murray also offers a tip for patients who react to foreign objects (like Great Lakes Dental Technologies’ George Gauge or Airway Metrics bite blocks) by shifting their jaws. He advises first watching how a patient naturally opens and closes before taking a bite scan, since a subset will show jaw deviation. For most, simply removing and reinserting the bite gauge allows them to settle into a more natural position once they’re familiar with the sensation, improving midline bite accuracy.
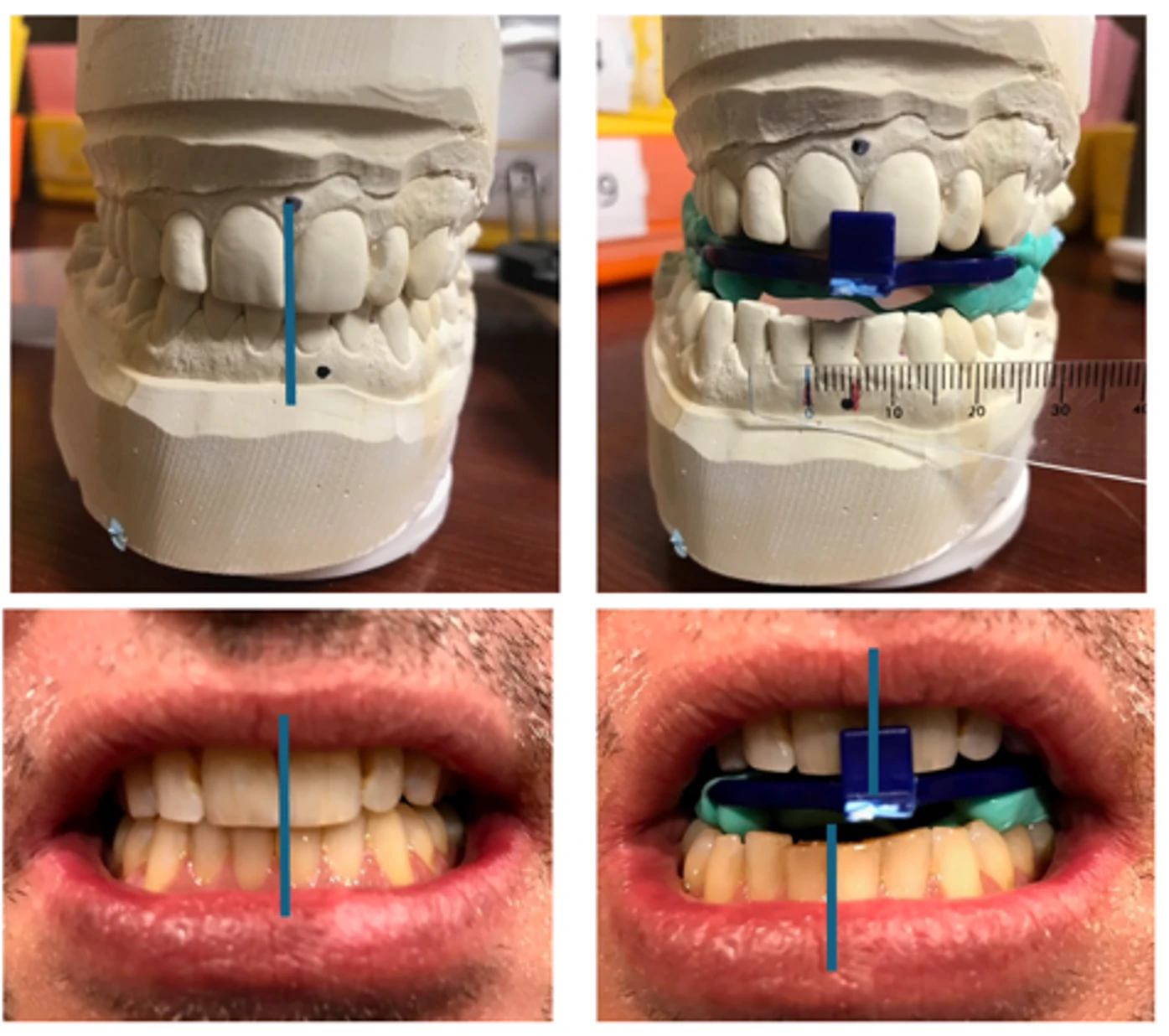
Michael Murray, DDS, DABDSM, founder of The Sleep Apnea Center of Connecticut, has developed a protocol to catch midline bite errors before sending digital scans to the lab.
‘Rapid Dose Titration’
Once an oral appliance is delivered, titration can begin. Most of Tozzer’s patients are optimally titrated within a month, down from the previous three- to four-month timeframe, courtesy of a new “rapid dose titration model,” which he presented at AADSM and SLEEP 2025. Using the Belun Tech home sleep testing (HST) ring and the ProSomnus EVO oral appliance, the time averaged 27 days from the records appointment to a confirmed therapeutic position.2
In Tozzer’s protocol, patients are fitted with their appliance and given a Belun Ring—a photoplethysmography (PPG)-based HST. Patients are instructed to advance their device 1 mm on each of five nights while wearing the ring. This data-driven approach allows Tozzer to identify the “sweet spot” in as little as five to seven days. Since his data shows that over-titrating can actually cause efficacy to degrade, objective data from the ring facilitates identification of a patient’s narrow range of optimal protrusion.
Patients with severe obstructive sleep apnea take longer (more EVO trays must be ordered), as do patients with TMJ disorders, who are advised to advance their oral appliance more slowly than patients with healthy TMJ.
“The value of the HST is that we can test them while we’re titrating,” Tozzer says. “We have about 14 Belun rings, and patients check them in and out like library books.” Out-of-area patients mail the ring back (in a hardshell camera box Tozzer bought off the internet) for $8 shipping.
Charles Tozzer, DDS, co-owner of Sleep Apnea Centers of California, developed a “rapid dose titration model” for oral appliances.
The shift toward faster titration has been facilitated by the emergence of PPG-based HSTs, observes Michael Cowen, CEO and founder of Awaken to Sleep and sister company HST Interps, which has seen the number of titration report orders from dentists increase exponentially since PPG technology debuted.
“I did not see anyone attempting rapid titrations prior to this,” Cowen says, adding that low price points and cloud storage of sleep study data have been game-changers. “Technology and financial friction points have been resolved by the technology that’s out there now.”
He recommends the EnsoHST with Viatom Checkme O2 Max as one great option for dentists. “Within roughly 15 minutes post the patient ending their test, EnsoHST will AI-score the data, create a template report based on our pre-saved tokens with the practice’s logo on it, and present that as a titration report,” Cowen says. “Dentists are getting great data through a validated source and then putting that on a silver platter in front of the physician.”
Monitoring Mandibular Jaw Movements Nightly
Alternatively, other clinicians prefer mandibular jaw movement HST for faster, “smarter” oral appliance titrations.
Jean-Benoit Martinot, MD, head of the Sleep Service and Laboratory at the Université Catholique de Louvain in Belgium, has studied the Sunrise HST, a mandibular jaw movement-based system, during oral appliance titration.3
For Martinot, the value of this approach is not just speed. “By faster, I mean smarter,” he says. Mandibular jaw movement analysis enables convenient, phenotype-aware monitoring nightly at home. Combined with patient-reported outcomes, this allows clinicians to titrate oral appliances in small increments while directly observing physiologic response.
Martinot appreciates Sunrise’s proprietary metric “REMOV,” defined as the percentage of sleep time spent with increased respiratory effort—which he posits adds a more comprehensive picture of residual disease burden and treatment response.
Nightly monitoring also reveals a non-linear dose-response curve, with rapid early improvement followed by diminishing returns. This helps clinicians avoid unnecessary over-titration and instead target the minimal effective protrusion—a strategy that may improve comfort, reduce side effects, and support long-term adherence. “Most of the time, just 60% of the maximum advancement is enough to obtain a significant effect,” Martinot says.
Equally important, mandibular jaw movements provide a real-world assessment of therapy effectiveness across multiple nights, capturing variability related to sleep stage and position. “We don’t need a long trial-and-error period,” Martinot says. “We can see very quickly whether a given position is physiologically effective.”
In that sense, faster titration is not simply about efficiency—it reflects a shift away from subjective, episodic assessment toward continuous, data-driven decision-making.
Scalability of Telemedicine
To further accelerate the path, some dentists are integrating telemedicine into their workflows. This approach addresses the common delay in obtaining a diagnosis and prescription from local sleep physicians who may have long wait times.
Sending patients with a high likelihood of sleep apnea to a national telemedicine physician appointment can streamline the diagnostic phase. Once the telemedicine service confirms the diagnosis and provides a prescription, the patient is referred back to the dentist for the oral appliance. Ashley Spooner, DDS, DABDSM, owner and general dentist/dental sleep medicine provider of Falcon Park Dental Group and the founder and CEO of Dynamic Dental Sleep, LLC, reports that approximately 80% of her referrals now come via Arima Health, a telemedicine pathway. “It just helps me to take that patient from identifying that they could have a problem all the way through that process,” she says.
This model not only speeds up the initial phase but also ensures that the dentist is working within a collaborative medical framework. The telemedicine physicians provide the necessary oversight and the final efficacy sign-off, allowing the dentist to focus on the technical aspects of appliance titration.
Convenient Patient Education
Of course, a fast titration is of little value if the patient discontinues therapy due to a lack of understanding or minor side effects.
Patient education is essential for success, as repetition ensures patients understand how to use repositioners and clean their devices. Dana Blalock, DDS, owner of Sleep Better South Carolina, utilizes a custom booklet she curated to address sleep hygiene and common troubleshooting issues without needing extra chair time. “Repetition is very important,” Blalock says. “We still have patients come back for follow-ups who will say, ‘Oh, what’s this morning repositioner for?’”
The approach of Blalock, who frequently orders devices by Panthera and ProSomnus for their “very good turnaround times,” includes repeating instructions during the delivery and having patients sign off on a delivery form. Her booklet covers everything from avoiding supine sleep to late-night exercise, providing a “gentle way” to remind patients that the appliance is only one part of their health journey. “The appliance works great, but it’s not going to improve every aspect of your life if you’re not trying to improve your health,” she adds.

Dana Blalock, DDS, owner of Sleep Better South Carolina, gives patients a booklet to address sleep hygiene and common oral appliance troubleshooting issues.
A Faster Future
Taken together, these approaches suggest that the time-consuming aspects of oral appliance therapy are less a limitation of the modality than of the workflows surrounding it. For those interested in implementing these protocols, Tozzer is optimistic that they will benefit practices.
“It did not degrade our success rate,” Tozzer says. “Patients are happier, referring doctors are happier, and even my front office staff is a lot happier because they’re not trying to force in so many appointment times. Our procedures are more standardized and go more smoothly.”
References
Murray M. A digital protocol to identify and eliminate construction bite errors. Sleep. 2025;48(Suppl 1):A343-4.
Tozzer C. Rapid dose titration model reducing treatment time in oral appliance therapy for OSA. Sleep. 2025;48(Suppl 1):A343.
Pépin JL, Cistulli PA, Crespeigne E, et al. Mandibular jaw movement automated analysis for oral appliance monitoring in obstructive sleep apnea: A prospective cohort study. Ann Am Thorac Soc. 2024 May;21(5):814-22.
Top photo: Ashley Spooner, DDS, DABDSM, owner of Falcon Park Dental Group, uses telemedicine to help speed patients through the sleep apnea treatment pathway.



